Het radiale tunnelsyndroom werd voorheen beschouwd als een mogelijke oorzaak van pijn die sterk lijkt op die van een tennisarm. De kans dat u een radiaal tunnel syndroom heeft is echter uiterst klein. In diverse onderzoeken wordt bevestigd dat een radiaal tunnelsyndroom als hoofdoorzaak van een tenniselleboog maar zelden voorkomt.
Echter als we kijken naar de (anatomie) aanhechting van de extensoren van de pols en de M. supinator op de laterale epicondyle lijkt er een een onlosmakende relatie te bestaan tussen de klassieke tenniselleboog zoals wij die kennen en het radiale tunnelsyndroom. Er zijn dan ook veel chirurgen die tijdens een tenniselleboog-operatie de lateraal epicondyle denerveren (Wilhelm’s denervation) en tevens decompressie van de radiaal tunnel uitvoeren.
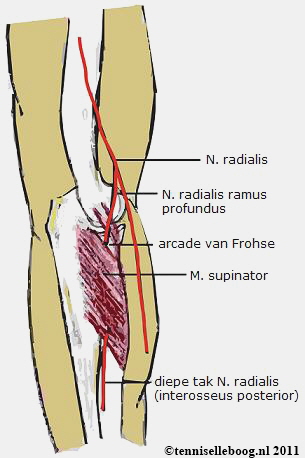
Een radiaal tunnel syndroom is een musculaire beknelling van de n. radialis die via de arcade van Frohse de m. supinator induikt (n.radialis ramus profundus ofwel n. interosseus posterior). De m. supinator is de meest waarschijnlijke oorzaak van dit syndroom, echter de n. radialis loopt niet bij alle personen door deze spier. De pijn is duidelijk in het verloop van de zenuw tot in de vingers te voelen.
De klassieke tenniselleboogtest geeft in principe geen vermeerdering van pijn. Wel kan het zijn dat tijdens actieve supinatie (naar buiten draaien van de onderarm tegen weerstand) of een volledige pronatie de pijn geprovoceerd kan worden. Een neurologische EMG geeft meer zekerheid over de diagnose.

Extra informatie voor wie meer wil weten
Radial Nerve Entrapment
Introduction
Radial nerve compression or injury may occur at any point along the anatomic course of the nerve and may have varied etiologies. The most frequent site of compression is in the proximal forearm in the area of the supinator muscle and involves the posterior interosseous branch. However, problems can occur proximally in relation to fractures of the humerus at the junction of the middle and proximal thirds, as well as distally on the radial aspect of the wrist.
Problem
Compression or scarring of the radial nerve at different points along its course may cause denervation of extensor/supinator muscles and numbness or paresthesias in the distribution of the radial sensory nerve (RSN). The result can be pain, weakness, and dysfunction.
Frequency
Among the problems associated with the 3 major nerves in the upper extremity, radial nerve entrapment is the least common. Carpal tunnel syndrome (median nerve compression at the wrist) and cubital tunnel syndrome (ulnar nerve compression at the elbow) are much more frequent.
Etiology
Radial nerve palsy
Radial nerve palsy in the arm most commonly is caused by fracture of the humerus, especially in the middle third (Holstein-Lewis fracture) or at the junction of the middle and distal thirds. The nerve may be compressed by the lateral intermuscular septum. This palsy may occur acutely at the time of the injury, secondary to fracture manipulation, or from a healing callus. Other less common causes of radial nerve palsy in the arm include compression at the fibrous arch of the lateral head of the triceps muscle and compression by an accessory subscapularis-teres-latissimus muscle
Radial tunnel syndrome
This diagnosis is highly controversial and is thought to be a result of overuse. Some authors believe radial tunnel syndrome may represent an early posterior interosseous nerve syndrome. Sites of compression include the fibrous bands attached to the radiocapitellar joint, radial recurrent vessels, the tendinous origin of the extensor carpi radialis brevis, the tendinous origin of the supinator (ie, arcade of Frohse), and fibrous thickenings within and at the distal margin of the supinator.
Posterior interosseous nerve syndrome
The etiology of posterior interosseous nerve syndrome is similar to that of radial tunnel syndrome. Compression is thought to occur after takeoff of the branches to the radial wrist extensors and the RSN. After emerging from the supinator, the nerve may be compressed before it bifurcates into medial and lateral branches, causing a complete paralysis of the digital extensors and dorsoradial deviation of the wrist secondary to paralysis of the extensor carpi ulnaris. If compression occurs after the nerve bifurcates, selective paralysis of muscles occurs, depending on which branch is involved. Compression of the medial branch causes paralysis of the extensor carpi ulnaris, extensor digiti quinti, and extensor digitorum communis. Compression of the lateral branch causes paralysis of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis proprius. Most commonly, entrapment occurs at the proximal edge of the supinator.
Other possible etiologies for posterior interosseous nerve dysfunction include trauma (Monteggia fractures), synovitis (rheumatoid), tumors, and iatrogenic injuries.
Wartenberg syndrome, described in 1932, is essentially entrapment of the superficial sensory branch of the radial nerve.
Many factors may contribute to the development of Wartenberg syndrome. In patients with de Quervain tenosynovitis, secondary irritation of the RSN is frequent. Other common causes include postsurgical injury, external compression, and trauma.
The anatomic site of compression corresponds to the transit of the nerve from its submuscular position beneath the brachioradialis to its subcutaneous position on the extensor carpi radialis longus. Especially with pronation, these 2 muscles can create a scissorlike effect compressing the RSN.
Presentation
Radial nerve palsy
Radial nerve palsy in the middle third of the arm is characterized by palsy or paralysis of all extensors of the wrist and digits, as well as the forearm supinators. Very proximal lesions also may affect the triceps. Numbness occurs on the dorsoradial aspect of the hand and the dorsal aspect of the radial 3 ½ digits. Sensation over the distal and lateral forearm is supplied by the lateral antebrachial cutaneous nerve and therefore is preserved
Radial tunnel syndrome
Radial tunnel syndrome is characterized by pain over the anterolateral proximal forearm in the region of the radial neck. This syndrome often appears in individuals whose work requires repetitive elbow extension or forearm rotation. The maximum tenderness is located 4 fingerbreadths distal to the lateral epicondyle, as compared with lateral epicondylitis, in which maximum tenderness is usually directly over the epicondyle. Symptoms are intensified by extending the elbow and pronating the forearm. In addition, resisted active supination and extension of the long finger cause pain. Weakness and numbness usually are not demonstrated.
Posterior interosseous nerve syndrome
Patients with posterior interosseous nerve syndrome present with weakness or paralysis of the wrist and digital extensors. Pain may be present, but it usually is not a primary symptom. Attempts at active wrist extension often result in weak dorsoradial deviation due to preservation of the radial wrist extensors but involvement of the extensor carpi ulnaris and extensor digitorum communis. These patients do not have a sensory deficit.
Rarely, compression of the posterior interosseous nerve may occur after bifurcation into medial and lateral branches. Selective medial branch involvement causes paralysis of the extensor carpi ulnaris, extensor digiti quinti, and extensor digitorum communis. With compression of the lateral branch, paralysis of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis proprius is noted.
Wartenberg syndrome
Patients with the diagnosis of Wartenberg syndrome complain of pain over the distal radial forearm associated with paresthesias over the dorsal radial hand. They frequently report symptom magnification with wrist movement or when tightly pinching the thumb and index digit. These individuals demonstrate a positive Tinel sign over the RSN and local tenderness. Hyperpronation of the forearm can cause a positive Tinel sign. A high percentage of these patients reveal physical examination findings consistent with de Quervain tenosynovitis.
Indications
Radial nerve palsy
Immediate exploration of a palsied nerve following a closed fracture of the humerus is contraindicated. A period of expectancy is indicated for 6-12 weeks to allow swelling and the palsy to subside. With a palsy developing after a closed manipulation, a further gentle remanipulation is carried out. Open exploration is indicated if there is no relief of the palsy or if it is felt that the nerve may be entrapped between the fracture fragments. In an open fracture or with a gunshot wound to the humerus with an associated palsy, exploration of the nerve at the time of debridement, as well as possible fixation, is the treatment of choice.
Radial tunnel syndrome
In radial tunnel syndrome, prolonged conservative treatment is indicated if the only symptom is pain. If pain does not resolve after 12 weeks, surgery may be indicated.
Posterior interosseous nerve syndrome
In posterior interosseous nerve syndrome, institute conservative treatment for 6-12 weeks. Surgery is indicated if no improvement occurs or paralysis increases.
Wartenberg syndrome
Wartenberg syndrome is best treated nonoperatively. Local application of steroids or iontophoresis is used. Nerve decompression is indicated only in resistant cases.
Relevant Anatomy
The radial nerve is the largest branch of the brachial plexus and is the continuation of the posterior cord, with nerve fibers from C6, C7, C8, and, occasionally, T1. The radial nerve innervates the extensor and supinator musculature located in the arm and forearm and provides distal sensation. Its course carries it across the latissimus dorsi deep to the axillary artery. It passes the inferior border of the teres major, winds around the medial side of the humerus, and enters the triceps muscle between the long and medial heads. It follows the spiral groove of the humerus, piercing the lateral intermuscular septum (10 cm proximal to the lateral epicondyle) from posterior to anterior, and runs between the brachialis and brachioradialis to lie anterior to the lateral condyle of the humerus.
Branches to the brachioradialis and extensor carpi radialis longus are given off just proximal to the elbow. The anconeus receives a branch from the radial nerve as well. The nerve then divides into a superficial branch and a deep branch. The extensor carpi radialis brevis may receive its innervation either from the radial nerve proper or from the posterior interosseous nerve. The superficial branch, which is purely sensory, runs under cover of the brachioradialis in the forearm. Eight centimeters proximal to the tip of the radial styloid, the nerve pierces the fascia medial to the brachioradialis to lie dorsal to the extensor tendons. It divides into a medial branch and a lateral branch to innervate the radial wrist (with some variable overlap from the lateral antebrachial cutaneous nerve), dorsal radial hand, and dorsum of the radial 3.5 digits (to approximately the middle phalanx level).
The deep branch of the radial nerve, the posterior interosseous nerve, winds to the dorsum of the forearm, around the lateral side of the radius, and through the muscle fibers of the supinator. It then divides into medial and lateral branches, each of which supplies different extensor muscles.
Abstract The most superior part of the superficial layer of the supinator muscle is named as the arcade of Frohse (AF). The deep branch of the radial nerve runs under this arch. The AF is reported to be the most common structure causing entrapment neuropathy of the deep branch of the radial nerve. The aim of our study was to reveal the anatomical properties and especially morphometric measurements of the AF in cadavers. This study was performed on 55 cadaver upper extremities. The AF was classified macroscopically as either tendinous or membranous. The width, length and thickness of the AF were measured as the dimensions of the AF. The distance AF between the lateral epicondyle of the humerus and the AF was measured. The forearm length between the lateral epicondyle of the humerus and the styloid process of the radius was measured. The distance AF was divided by the forearm length to find the ratio AF. In 87% of the extremities the AF was tendinous, and in 13% it was membranous. The mean width, length and thickness of the AF were 10.13, 8.60 and 0.77 mm, respectively. The mean distance AF and forearm length were 46.23 and 233.17 mm, respectively. The mean ratio AF was 0.199 (approximately 1/5). These measurements of the dimensions of the AF may contribute to the anatomy of the AF. The surgeon may find the predicted distance AF of any upper extremity by dividing its forearm length by 5.